Extra articular – better prognosis
Intra articular – worse prognosis
- >75% of all calcaneal fractures
Rowe
- Mainly for extra-articular fractures
-
Type I
-
A -
Fracture of the tuberosity of the calcaneus
- Best visualized on axial views
-
Always secondary to shearing forces
- Calcaneus is at an angle and forces shear off the tuberosity
- May be due to avulsion of plantar structures – fascia, intrinsic muscles
- If small and not grossly displaced do not need to be fixed
- If large or grossly displaced they need fixation
-
B -
Sustentaculum Tali Fracture
- Best seen on axial view
- Hallmark – pain with motion of FHL tendon, right under sustentaculum tali
- Shear type fractures
- May be avulsion from eversion sprain – deltoid ligament pulls of sustentaculum
- Don’t need to be fixed if in good approximation
- If grossly displaced they need fixation
-
C -
Fracture of the Anterior Process of the Calcaneus
-
2 main causes
- Avulsion from bifurcate ligament or EDB
- Compaction when there is dorsiflexion and inversion of the foot and the lateral talar process impacts the anterior process into cuboid
-
2 main causes
-
A -
Fracture of the tuberosity of the calcaneus
-
-
- If intra-articular and large they should be fixated for early motion and reduced chance of DJD at CC joint
-
-
Type II
- Fracture of posterior superior aspect of calcaneus
-
A -
Beak Fracture
- Dorsal 1/3 of tuberosity
- Shear or blunt trauma
- Lateral x-ray
- Don’t fix if small and non-displaced, just cast
- If large or displaced it needs fixation
-
B -
Avulsion Fracture at insertion of the achilles tendon
- Achilles avulsion – middle 1/3 of calcaneal tuberosity
- Often caused by dorsiflexion forces of foot
- Usually need fixation
- AK cast if well approximated
- If long standing (>3 weeks) they may need TAL or gastroc recession to get fragment down
-
A -
Beak Fracture
-
Type III
- Oblique Fracture of the Calcaneal Body NOt Involving the STJ
- Cast if not grossly displaced, if grossly displaced then it needs fixation
- Usually heal well due to vascularity of calcaneus
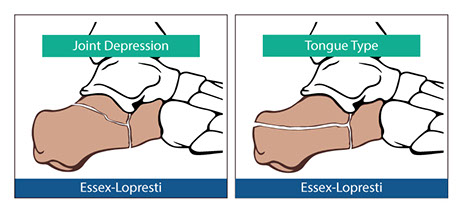
- Type IV - Intra-Articular Fractures Involving the Subtalar Joint (tongue-type - Essex-Lopresti)
-
Type V
- Intra
-Articular Central Depression with Varying Degrees of Comminution (joint depression - Essex-Lopresti)
- Depression of posterior facet into main body of calcaneus
- Severely comminuted
Essex-Lopresti - X-ray based classification
- Used for intra-articular
-
Tongue Type
- non- Joint depression
- Like Rowe Type IV
-
Joint Depression
- Like Rowe Type V
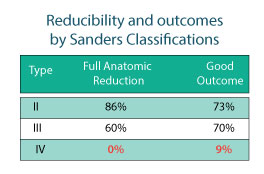
Sander's - CT classification (coronal)
- Number of fracture lines
- BEST - gives an idea of the type of clinical outcome and the ease of reducibility
-
Type I
- all non-displaced articular fractures, regardless of the number of fracture lines present
- No fractures through the posterior facet
- Type II - 2 part articular fracture of posterior facet - 1 fracture line
- Type III - 3 part articular fracture - Two fracture lines
- Type IV - 4 part articular fracture - Three fracture line
- Further classified into location of fracture lines
-
- A - Lateral fracture line
- B - Central fracture line
- C - Medial fracture line - Sustentaculum Tali Fracture
-
Reduction Criteria
for Sander’s Fractures:
-
Anatomic Reduction
- No incongruity in joint surface of posterior facet
-
Near
Anatomic Reduction
- <3 mm incongruity of joint surface of posterior facet
- An acceptable level of reduction
-
Approximate
Anatomic Reduction
- 3-5 mm incongruity of joint surface of posterior facet
-
Failed
Anatomic Reduction
- >5 mm incongruity of joint surface of posterior facet
-
Anatomic Reduction